Shockwave Therapy
Shockwave Therapy
Act - Conditions
- Lateral epicondylitis/ lateral epicondylalgia - Tennis elbow
- Calcific Tendonitis - Rotator Cuff Tendonitis
- Epicondylitis - Golfer's Elbow
- Myofascial TriggerPoint - Chronic Deep Tissue Muscle Pain
- Patellar Tendonitis-Jumper's Knee Tendonitis
- Trochanteric - Hip Tendonitis
- Achillodynia- Achilles Tendonitis
- Tibial Stress Syndrome - Shin Splints
- Plantar Fasciitis - Heel Spur
- Scar tissue treatment
- Morton' Neuroma
- Iliotibial Band Syndrome
- Treatments for non-healing ulcers
- Hamstring Tendonitis
- Neck, shoulder, back, and hip pain
Acknowledgments
Reporting checklist: Authors have reviewed the STROBE reporting checklist. Available at http://dx.doi.org/10.21037/tau-20-911
Data Sharing Statement: Available at http://dx.doi.org/10.21037/tau-20-911
Peer Review File: Available at http://dx.doi.org/10.21037/tau-20-911
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tau-20-911). DAS is an unpaid member of the editorial board for Translational Andrology and Urology, from December 2017 through July 2022. DAS reports investment from Triurol, paid consultant from UroGen, outside the submitted work. The other authors have no conflicts of interest to declare.
Ethical Statement. The authors must ensure that all questions regarding the integrity or accuracy of any portion of their work are properly investigated and solved. The study was conformed to the provisions of the Declaration of Helsinki (as revised in 2013). This study was reviewed and approved by the Cleveland Clinic Institutional Review Board (IRB No. 12-118). Informed consent was waived for this retrospective study as no direct interventions to the patient were present.
Open Access Statement: This is an Open Access article distributed in accordance with the Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License (CC BY-NC-ND 4.0), which permits the non-commercial replication and distribution of the article with the strict proviso that no changes or edits are made and the original work is properly cited (including links to both the formal publication through the relevant DOI and the license). See: https://creativecommons.org/licenses/by-nc-nd/4.0/.

Shock Wave Facts And Features
High-energy, audible sound waves called shock waves can be heard. In the medical world, Shock waves have been employed since around 1980 in a process called Lithotripsy to disintegrate kidney stones.
Modern musculoskeletal pain therapy uses Shock Wave energy. It is produced by the Shock Wave device and transmitted through the handpiece. The shock wave energy stimulates the body's intrinsic healing abilities to heal damaged tissue.
More recently there has been a plethora of new uses discovered for this therapy from, improved wound healing to cartilage regeneration, cellulite reduction and anti -wrinkle facial skin regeneration. This therapy method is used to treat racehorses for their tendon injuries. This technology is still being explored.
Study Limitations
Risk of bias scores for RCTs were 60% and 74% respectively, which indicates a high level of risk. The lowest scoring items were participant blinding, allocation concealment and study size calculation. Other sources of bias, as defined by imaging assessment accuracy, also received low scores. Of particular interest to this review, the accuracy of imaging measurements was questionable in some cases due to the under-reporting of details pertaining to measurement standardization. It was decided that meeting a minimum of two out of an a priori set of four criteria related to imaging accuracy would be used for judging risk of bias based on imaging accuracy. This criteria was based upon providing information about the skills and experience of the radiologists in musculoskeletal image, the details of the procedure for imaging accuracy to assure participant's consistency during each image acquisition, previous testing or training by the assessor, as well reporting the scores of measurements that are based on multiple measurements.
The innovative treatment of various musculoskeletal disorders with shockwave therapy is a new method. It can be used when traditional therapies have failed. The therapy can be considered non-invasive and low-cost. It is also free from the risks of surgery and any postoperative pain.
The exact mechanism behind ESWT's action is still unknown. However, shock waves can trigger stimulations which activate small-diameter fibers. This activates a serotoninergic network that controls the transmission of pain stimuli, increasing the patient’s tolerance to pain above the original. Additionally, ESWT causes a localized metabolic reaction, due to increased vascularity and less formation of adhesions, which occur in promoting the natural healing process (7).

Benefits
Dr. Finnoff notes that this approach fills a need for athletes whose injuries are not responding to first line treatments, such as rest, ice, therapeutic exercise, bracing and orthotics, but who are not yet ready to consider more-invasive or surgical options.
Dr. Finnoff explains, "Say that we're treating a middle-of-the season basketball player who has jumper's injury to his knee which is preventing him or her from practicing or playing." After all other non-operative options have failed, ESWT may be an option. We usually tell athletes that they have had to stop playing after they have tried all the non-operative treatments. If they have not been successful, they are told that they may need more invasive treatment such as needle tenotomy or experimental regenerative medicine. All of these options have higher risks, longer recovery times, and have higher cost. While often successful, all of those more-invasive therapies require time off and can effectively end an athlete's season. ESWT provides an excellent option for athletes that can be used if they are successful and doesn't end their season.
Shockwave Therapy
Dr. Berry was the first doctor in Southern California who offered shockwave therapy.
LISTEN TO THIS PATIENT TALK ABOUT HIS FROZEN SHOULDER AFTER ONLY ONE TREATMENT!
The use of shockwave therapy in rehabilitation and orthopedic medicine is relatively new. The effect of shockwaves was first documented during World War II when the lungs of castaways were noted to be damaged without any superficial evidence of trauma. The internal injuries were caused by shockwaves from depth charges. This created a great deal of interest and research into the biological effects of shockwaves on living tissue. The first medical treatment developed from this research was lithotripsy. This technology allowed for focused shockwaves that could effectively dissolve kidney stones, without the need to have surgery. This technology is used to treat over 98% all kidney stones. The use of shockwaves to treat tendon related pain began in the early 1990s.
THIS PATIENT HAD ANKLE AND FOOT PAIN FOR OVER TWENTY YEARS! GONE WITH ONE TREATMENT
Clinical shockwaves are nothing but controlled explosions that produce a sound pulse. It is similar to an aircraft breaking through the sound barrier. The primary effect of a shockwave is a direct mechanical force. It is unknown how shockwave therapy works to relieve tendon disease. The leading explanation is based on the inflammatory healing response. The shockwaves can cause microtrauma in the tendon tissue. This results in inflammation, which allows the body to send healing cells and increase the blood flow to the injured site.
KNEE PAIN - THIS PATIENT HAD KNEE PAIN FOR MORE THAN ONE YEAR.
The patient had been limping for 2 weeks and was suffering from severe shin splint pains.

More Results
The treatment of 48 men suffering from ED that met our criteria was SWT. 24 were given fSWT, 24 had rWT. Patients were 65.6 years old (IQR 51-70), had a median pre-treatment SHIM of 8 (IQR 5-13), and used PDE5i for 85%. The baseline characteristics for each cohort are shown in Table 1. There was no statistical difference between the fSWT and rWT groups in age (61.3 vs. 60.5 years), duration of ED symptoms (61 vs. 72 months), pre-treatment use of PDE5i (79% vs. 92%), or the baseline SHIM score (9.3+-4.2 vs. 9.3+-4.8). All patients completed their 6-week treatment course. All patients had pre- and post-treatment SHIM scores and no missing data or loss to follow-up requiring imputation.
Figure 1 shows that there was an increase in SHIM scores for both modality at 6 weeks after treatment (Figure 1). The mean SHIM of patients treated by rWT improved from 9.3 to 16.1 (SD 5.9) (P<0.0001). Similar results were seen for patients who received fSWT. The mean SHIM improved from 9.3 to 16.1 (SD 5.9) (P0.0001). The delta SHIM was not statistically different between fSWT and rWT (P=0.42 Figure 2).
25 percent of men who were treated with rWT reported no improvement in their erections (grade 1) while 42% (grade 2) reported adequate penetration using PDE5i(grade 2) and 33% (grade 3) reported that they had sufficient erections to avoid the need for PDE5i (3rd grade). The fSWT treatment group had 46% (grade 1) and 17% (grade 2) who reported that they experienced sufficient penetration using PDE5i. Meanwhile, 37.5% (grade 3) reported adequate erections with no need for PDE5i. In the rWT group, 75% (18/24) had a >= grade 2 response compared to 54% (13/24) in the fSWT group; however, this was not a statistically significant difference (P=0.42).
None of the patients included in this study experienced an adverse event.
This study shows that shockwave therapy resulted in a substantial reduction in pain and an improvement in functionality and quality in life for patients with plantar fasciitis and Achilles tendinopathy. Significant pain reduction and improvement in functionality and quality of life were also observed in the control groups of each tendinopathy, but these findings were less pronounced than those in the group treated with shock waves.
It is not possible to compare the results of other studies because of differences in the devices used, the mechanisms that produce shock waves and the energy flux utilized. The present study showed that shockwave therapy was able to produce similar results in patients with plantar fasciitis and elbow tendinopathy as in previous studies.
Numerous studies have examined the effects of shockwave therapy on plantar fasciitis. The results showed significant alleviation of pain and improvement in functional ability immediately after the treatment and these findings continued during the entire follow up of 3, 6 and 12 months (4, 8). Othman and Ragab (9) applied shock waves of energy intensity from 17 to 21 kV, 2 Hz and 1,500-3,000 pulses and showed a marked improvement in pain and 50% of the patients had no limitation of activities after the 6 to 11 month follow-up. Other researchers (10) applied high energy of shock waves (1,500 shocks with total energy of 324.25J) and showed improvements in pain and functionality which was maintained between week three and twelve post-intervention, and continued to a lesser extent for up to one year. One other study (11), also found significant pain relief immediately following treatment, and three-month- and twelve-month-long follow-up.
Evidence supporting our findings has been also found in the case regarding elbow tendinopathy. Spacca, Necozione and Cacchio (12) assessed pain using the VAS scale and functional impairment using the DASH questionnaire. Radial shockwave therapy was used. Each session contained 2,000 impulses. They found a statistically significant reduction (improvement) in pain and functional impairment after the completion of the therapy and the 6-month follow-up compared to pain before treatment. Ilieva, Minchev and Petrova (13) also used radial shockwave therapy of 2,500 impulses and performed a total number of 5 treatments one per week. There was a marked difference in the pain scores between before and after treatment. This decrease was maintained at three, six and twelve months. The pain, function and the total score as assessed on the patient-rated scale (PRTEE) also showed statistically significant improvement after completion of therapy and at the 3, 6 and 12 month follow-up. Melikyan et al (14) also showed a significant decrease in the DASH function/symptom score, which reflects to an increase in functional level, after the 1, 3 and 12 month follow-up. Other studies, also found significant improvement with respect to the reduction of pain, functional scale and patient activity score not only post-treatment but also after a 12 week follow-up and in comparison to placebo (15, 16).
ESWT is also effective in the treatment of Achilles tendinopathy as it has been confirmed by some randomized controlled trials. Rasmussen et. al (17) found that there was an improvement in activity and function after ESWT therapy. These improvements were more evident at 8 and 12 weeks follow-ups. This is measured using the AOFAS score. It measures subjective pain and function as well as objective scores based upon a physical exam. Lakshmanan (18) and O'Doherty (18), treated Achilles tendinopathy with 3 sessions of radial shockedwaves, each lasting one week. Each session consisted of 2000 impulses of radial shatter waves at 2.5 bar pressure, with a frequency between 6-10 Hz and included 2.5 bar of pressure. Results showed that there was a decrease in mean VAS pain scores (p0.001) and an improvement following treatment. The VISA-A score, which analyses the function of the Achilles tendon, also significantly improved after the treatment (p<0.001). Rompe and colleagues (19) found a significant improvement in VISA-A scores, which measure pain function, activity, and function, both at the end of therapy and during the follow-up period.
Numerous studies have examined the effects of ESWT upon the tendinopathies in the rotator-cuff. Wang and colleagues (20) observed significant improvements in pain intensity, activity, and motion following treatment with 1000 impulses of shock waves. This improvement continued for three, six, or more sessions. Rompe et al (21) also found similar results in shoulder functionality at 6 and 24 weeks after treatment by using a single session of 1,500 impulses. Accordingly, Cosentino et al (22) found a significant improvement in pain, daily activities and range of motion by applying 4 shockwave sessions of 1,200 shocks after the treatment and the follow-up evaluations at one and six months using a VAS and Constant-Murley score. Hsu et al (23) showed significantly better results in both pain reduction and improvement of function measured by the Constant-Murley score after administration of a high-energy shockwave. Cacchio et al (24), reported a study that used high-energy shockwaves instead of sham therapy. Significant reductions in pain and improvements in function were observed from four weeks to six months. Other studies assessed high energy ESWT versus low energy ESWT and comparisons between them and a placebo were estimated. Significant relief in pain and a greater increase in the functional outcome were seen in both high energy and low energy ESWT compared to control treatment at 3 and 6 months post-treatment, but significantly better results were seen in high energy treatment (3, 25-27).
Extracorporeal shockwave treatment is proven to be effective in relieving the pain and increasing functionality in several tendinopathies, including plantar fasciitis and Achilles tendinopathy. The therapy can be performed outpatient with no restrictions on patients and has no side effects. The current research shows that extracorporeal shockwave therapy is safe and effective in treating all types of tendinopathies. Thus, patients who failed to respond to conventional treatment for any of the above tendinopathies can use shockwave therapy as an alternative method, which can significantly improve pain, functionality and quality of life.
There may have been differences in ESWT effectiveness in various tendinopathies. These could be due to differences in research designs and populations. To determine the optimal parameters for shockwave therapy's efficacy, further research is needed.

One Of The Few Clinics In The Country To Offer Extracorporeal Magnetotransduction Therapy (Emtt) Along With Both Focused And Radial Shockwave Therapy!
Kent Chiro-Med are happy to offer EMTT in Ottawa. We also offer both Radial and Focused Shockwave therapy as a highly effective modality for the treatment of neuromuscular disorders and injuries while being non-invasive. Shockwave Therapy, which has been approved by FDA since 1995, is used throughout Europe.
EMTT was approved by FDA in the USA for use for 6 months. However, it has been used successfully in Europe for 3 years.
The highly efficient technology of shockwave uses electro-magnetic or /or son waves to activate the body's natural reparative response, enhancing neovascularization as well as collagen production.
What Should I Expect During Shockwave Treatment?
The shockwave treatment of plantar fasciitis and heel spurs or chronic tendinopathy only takes five minutes. Your provider applies a special gel to your skin and uses a state-of-the-art machine to emit sound waves into injured or painful areas of your foot or ankle.
You might feel slight discomfort during treatment, but most patients tolerate it well. Your doctor adjusts the soundwave applicator's intensity to make your experience as comfortable as possible.
Shockwave therapy is not invasive and does not require a long recovery time. You can return to your normal activities immediately after treatment. For best results, your podiatrist may recommend that you have 3-5 sessions spaced between 3-10 days. However, many people feel relief within a single session.

What Is Shockwave Therapy?
The clinical term for shockwave therapy is low-intensity shockwave therapy (LiSWT). This noninvasive treatment has been used for many years in orthotics to heal fractures and ligaments.
LiSWT can also be used to speed up wound healing. Using targeted high-energy sound waves, LiSWT can speed up tissue repair and cell growth.
Erections rely on healthy blood flow to the penile tissue. Shockwave therapy is viewed favorably as a way of repairing and strengthening blood vessels in the penis and improving blood flow.
Increasing blood flow to the penis is the same goal of more traditional ED treatments, such as oral medications, including sildenafil (Viagra) and tadalafil (Cialis).
Conclusions:
Shockwave therapy significantly reduced the pain that accompanies tendinopathies and improves functionality and quality of life. Because of its safety and effectiveness, it might be the first option.
Extracorporeal Shockwave Therapy (ESWT) was first introduced into clinical practice back in 1980 as a treatment for non-invasive lithotripsy (1). It has also been utilized for the treatment of musculoskeletal conditions and stimulation of bone growth over the past two decades (2). Thus, the shock waves are used for the treatment of various orthopedic conditions including plantar fasciitis, shoulder tendinopathy, elbow tendinopathy, patellar tendinopathy and Achilles tendinopathy (3-5). Recently, shockwave treatment has been extended to treat other conditions, including femoral head necrosis, patellar knee jaw, osteochondritis and calcified shoulder tendonitis.
High energy sound waves, also known as shock waves, are produced in water by high-voltage explosions and evaporation. In the case of lithotripsy, shock waves are used to dissolve nephrolithiasis while in orthopedic cases they are used to induce neovascularisation at the junction of the tendon-bone and the release of growth factors such as eNOS (endothelial nitric oxide synthase), VEGF (vascular endothelial growth factor) and PCNA (proliferating cell antinuclear antigen). These stimulate cell proliferation, improve blood flow and eventually lead to tissue repair by allowing for the regeneration of bone and tendons.
The shockwave therapy is an innovative non-invasive treatment that does not involve a surgery and doesn't cause any pain.
The purpose of this study was to record the pain, functionality and quality of life in individuals suffering from various tendinopathies and subsequently to investigate the pain reduction, the improvement in the patient's functionality and quality of life both immediately and 4 weeks after therapeutic intervention with shock waves. Comparisons between shockwave intervention groups and controls were made.
Researchers Population: This sample included 384 tendinopathy patients (58 in the shockwave intervention and 226 in the control) who were seen at an orthopedic clinic between February 2015 and December 2016. The physician assessed their needs and recommended the appropriate treatment. The conservative treatment for patients in the control group included the application of NSAIDs as gels or creams locally, support straps, a program of exercise depending on their tendinopathy, modifications to activity, friction massage and the placement of hot and cold packs on any injured areas. There were four tendinopathies that we examined: plantar fasciitis (elbow tendinopathy), Achilles tendinopathy (achilles tendinopathy), and rotator-cuff tendinopathy.
Exclusion criteria: Patients under the age of 18 were excluded from the study. Research Tools: A self-administered anonymous questionnaire was created bearing the name 'University of Peloponnese Pain, Functionality and Quality of life Questionnaire-UoP-PFQ'. The questionnaire consisted of four parts. Both the first and second sections were filled out by patients in both the groups prior to the start of therapy. The first part was related to the demographic characteristics of the patients, whereas the second part was further subdivided into three sections, one for the evaluation of the perception of pain upon precise movements on a five-point Likert scale where 0=no pain, 1=low pain intensity, 2=medium pain intensity, 3=high pain intensity and 4=severe pain intensity. The second part examined functionality and movements in the lower and upper limbs. Finally, the third section evaluated the quality of life. It used a 5-point Likert scale to assess the difficulty of performing daily tasks on the five-point scale. Doctors completed the third section of the questionnaire. It contained information from the medical evaluation, such as diagnosis, pain reports, type of treatment and number of sessions. The fourth section of the questionnaire, which was identical to part 2, was filled out by both patients in the two groups. It was done immediately following the end of treatment (post-treatment), and the subsequent 4-week follow up.
The internal consistency of the questionnaire (Cronbach's alpha coefficient) was equal to 0.88.
Parameters of shockwave therapy: The patients were shocked using a STORZ MEDICAL MP200 device and the following parameters.
Elbow Tendinopathy: For the initial session, the frequency was set to 21 Hz, the pressure at 1.8 bar and 2000 shocks to achieve analgesia. The frequency of the remaining sessions was changed to 15 Hz, with the pressure set at 1.6bar and 1500 shocks in order to obtain therapy.
Achilles tendinopathy: For the initial session, the frequency was set to 21 Hz, the pressure at 1.8 bar and 2000 shocks to achieve analgesia. For all remaining sessions, the frequency was set to 15 Hz, the pressure at 2.0 bar and 3000 shocks to achieve therapy. Plantar fasciitis: For the initial session, the frequency was set to 21 Hz, the pressure at 1.6 bar and 1500 shocks to achieve analgesia. The frequency of the remaining sessions was adjusted to 15 Hz. To achieve therapy, the pressure was at 1.8 bar with 2500 shocks.
Tendinopathy in the rotator wrist: The initial session was at 21 Hz. To achieve analgesia, pressure was set at 1.8 bar with 2000 shocks. To achieve therapy, all subsequent sessions were set at 15 Hz with a pressure of 1.8bar and 1500 shocks. Ethical concerns: The study was conducted in accordance with the ethical guidelines that guide research. More specifically, participants' information was kept confidential. The safety and anonymity of data was maintained. Only the study results were made available to them. Finally, the study protocol was in compliance with Helsinki Declaration and was approved by the University's Ethical Committee.
Is shockwave therapy really effective?
Provided you are a candidate for this type of treatment, clinical studies suggest there is an 90% - 95% success rate for this technology in treating patients with applicable conditions. Scientific research supports the use of ESWT Shockwave therapy in the treatment of tendinopathy, plantar fasciitis, calcifications and many other muscular-skeletal conditions.
It is crucial to be able to determine which conditions and patients are most likely for this therapy to work. Given our experience we believe we can provide you with an accurate assessment on your candidacy for Acoustic Wave Therapy and the likelihood you will see an improvement in your condition.
What Does The Research Say?
Shockwave therapy was found to significantly improve erectile function in the same meta-analysis and 2019 review. The best results were seen in men suffering from vasculogenic Erectile Dysfunction.
A 2010 pilot study found that among 20 men with vasculogenic ED, all experienced improved erectile function after 6 months of shockwave treatment. Follow-up with the men found no adverse effects.
Despite this encouraging research, the Food and Drug Administration (FDA) hasn't approved shockwave therapy as a treatment for ED. Although some doctors still recommend shockwave therapy to treat ED, it is not approved for use in a clinical setting.
FDA approvals for new treatments are always accompanied by guidelines for doctors to follow and side effects to be shared with patients.
As with any unapproved treatment, if you choose to do shockwave therapy for ED, there may be risks that aren't properly explained, or you may be spending money on a treatment that doesn't live up to its promises.
Additionally, treatments that haven't been approved by the FDA usually aren't covered by insurance.
According to a statement from the Sexual Medicine Society of North America (SMSNA), there isn't enough "robust clinical trial data" to support the widespread clinical use of shockwave therapy. The SMSNA recommends that shockwave therapy only be done under strict research protocols.

Is there any known side effects to shockwave therapy?
Treatment side-effects are limited to reddened skin and/or minor soreness at the treatment site.
Advanced Laser Therapy: What is it?
Advanced Laser Therapy uses photons to flood the tissues, which stimulate the injured cells and improve circulation. The body's natural healing response is activated, which reduces inflammation and can even eliminate your pain. Treatments take just a few minutes, and the therapeutic effect continues to soothe and heal long after you leave our office.

Are You Covered?
Shockwave therapy does not fall under the OHIP. It may be covered under some extended benefit plans, check with your provider.
Side effects and risks
Most men find shockwave therapy painless. And as previously stated, available research has found few, if any, side effects.

What are the best treatments to improve my condition?
The treatment frequency and duration depend on the specific condition being treated. After an evaluation, your Shockwave specialist can provide you with a detailed plan of treatment.
Advantages
- Alleviation of musculoskeletal pain
- Mobility improvements
- Non-invasive
- This reduces the use of pain medication
- Outpatient treatment
- Short therapy time of approx. 10-20 min.
- Focused patient-guided therapy
Call us TODAY at (613) 695-8600 to get a free consultation and find out if SHOCKWAVE Therapy is right for you
How Does It Work?
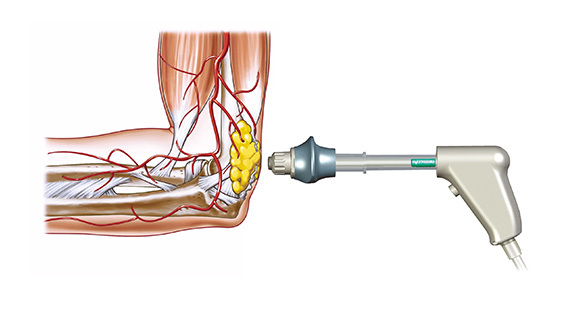
With Radial Shockwave Therapy a projectile accelerated in the handpiece generates a mechanical pressure wave which is transferred to the body via an applicator head for the purpose of reducing adhesions (scarring) in muscle, ligament, and tendon.
The difference: This isn't an electrical shock.
How Kidney Stone Extracorporeal Therapy works
Anesthesia prevents pain during the procedure. Two ways shock waves can reach the stones are:
- Water bath immersion -- You will sit in a tub of lukewarm water
- Soft cushion -- You will sit on soft cushions on top of a table
To locate the stone, your doctor may use X-rays and ultrasound. Your doctor will position your body accordingly and send shock waves through the stones until they're crushed into tiny pieces.

Results:
The pain reduction and the improvement of functionality and quality of life after shockwave treatment increased by at least two points on the five-point Likert scale both post-treatment (p<0,001) and at a 4-week follow-up (p<0,001) compared to post-treatment in elbow tendinopathy, Achilles tendinopathy, plantar fasciitis and rotator cuff tendinopathy.
Benefits Of Shockwave Therapy
Our patients receive many benefits from shockwave therapy:
- No significant side effects
- Safe for patients
- Surgery-free
- There are no patient restrictions
- There is no need for anesthesia
- No injections are needed
The therapy is not just effective for foot pain but also treats tissue, tendon and muscle issues in various areas. Shockwave therapy is also a great cosmetic and aesthetic option.